
While KAND is a neurodegenerative disease, it does not affect any two people the same way. Progression and severity of KAND varies by mutation, and some mutations are more common than others. Our leading research team at Chung Lab at Boston Children’s Hospital has evaluated over 330 families affected by KAND to understand the clinical features of this disease. If you have questions about KAND symptoms and how they affect you or a loved one, please contact the Chung Laboratory by emailing ASCENDstudy@childrens.harvard.edu.
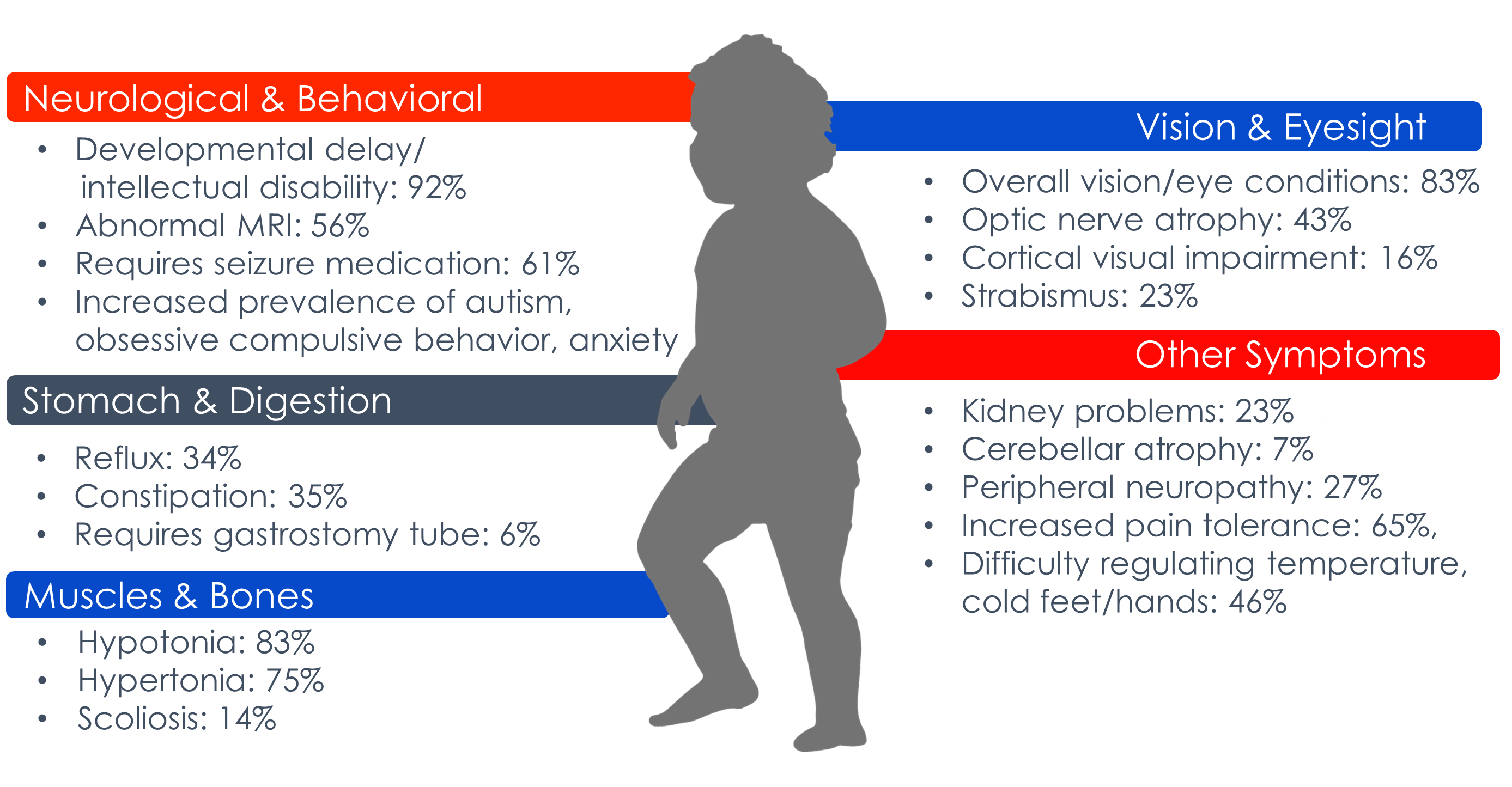
The following symptoms are commonly associated with KAND.
Introducing KAND to your Doctor? Bring our KIF1A Primary Care Physician guide with information on symptoms and resources.
Click on each section below to learn more about specific symptoms.
KAND patients experience many overlapping symptoms relating to muscle strength, coordination, reflexes, and balance. These symptoms may worsen over time as a result of degeneration, and increased strain as the body grows. Falls are a common source of broken bones in KAND.
Spasticity and hypertonia
Hereditary Spastic Paraplegia (HSP) refers to a group of degenerative disorders, characterized by spasticity of the legs and progressive muscle atrophy. Spastic Paraplegia 30 is the specific subtype grouped by KIF1A mutations.
HSP can be identified by gait abnormalities or limited range of motion in the legs. Spasticity causes jerky reflexive movements: Muscles’ stretch signals are amplified and cause overcompensated contractions, which can override intentional movement originating in the brain. The more forceful the initial movement the harsher the contraction, and this can cause feedback loops of spastic jerking during voluntary movement. KAND individuals often incorporate spasticity into their gait to generate force, which may mask weakness or muscle atrophy.
✨Check out our Spasticity in KAND page for more information.
Hypotonia
KAND patients may experience mixed muscle tone, with increased tone in their legs, and decreased tone in their core and arms.
Hypotonia is the medical term for low muscle tone. Infants and young children experiencing this symptom are often described as “floppy.” You may notice a child feeling limp when you hold them and showing less control of their neck muscles, causing the head to drop. It may also be difficult for them to place weight on their leg or shoulder muscles.
Ataxia
Ataxia is characterized by a lack of muscle coordination and balance, you may notice slurred speech, trouble eating and swallowing, rapid eye movements, deterioration of fine motor skills, difficulty walking (unsteady gait) and tremors. About half of KAND patients struggle with coordination.
Flat Feet
About half of KAND patients assessed in the natural history study had flat feet, which may result in further fatigue or risk of injury when walking.
Peripheral Neuropathy is caused by damage to your peripheral nerves, which carry information from your brain and spinal cord to the rest of your body. This symptom can involve numbness in the hands and feet, a stabbing, burning or tingling pain throughout the body, extreme sensitivity to touch, and a lack of coordination. KAND patients often exhibit reduced pain and temperature sensitivity, which may make them more prone to ignoring injury.
Unfortunately, vision conditions are one of the most common features of KAND, affecting 84% of patients. Symptoms include reduced visual acuity, compromised depth perception, reduced peripheral vision, and color blindness. Optic nerve atrophy, cortical visual impairment, and strabismus/nystagmus are all common.
Severity and progression vary widely between patients, but the most recent Natural History Study recommends“… regular assessments with a neuro-ophthalmologist to assess for optic nerve atrophy and cataracts that we have observed in some older individuals.” (Sudnawa et al. 2024, Genetics in Medicine).
✨Check out our Vision in KAND page for more information.
Almost half of KAND patients experience seizures, and epilepsy in KAND can vary widely by seizure type and frequency. Absence, Tonic-Clonic, Spasm, Atonic, and Simple/Complex Partial Seizures have all been observed. Additionally, background slowing of the EEG and/or epileptiform abnormalities were observed in 15/18 patient EEGs assessed in the KAND natural history study.
Some children affected by mutations in KIF1A experience Continuous Spikes and Waves During Sleep (CSWS). Seizure activity in KAND often occurs at night, and could go unnoticed during a routine EEG. Because this form of epilepsy is rare, overnight EEG monitoring helps diagnose and treat seizure types associated with KAND. Seizures that go unidentified and untreated can result in severe brain damage over time, and sometimes death.
“We report a high frequency of seizures and/or abnormal EEGs, similar to previous studies… KIF1A should be considered an epilepsy gene and that baseline EEG is warranted in newly diagnosed patients.” Sudnawa et al. 2024.
✨Check out our Epilepsy in KAND page for more information.
Intellectual Disability
Intellectual Disability (ID) most often results in developmental, speech and language delays in children. You may notice issues with verbal expression, difficulty expressing or receiving information, or problems with developing motor and fine-motor skills.
Autism
Mutations in KIF1A can also result in a clinical diagnosis of Autism Spectrum Disorder (ASD). We are still learning about the genetic causes of autism; however, characteristics of ASD include difficulty with altered sensory sensitivity, altered communication and interaction with other people, and restricted interests and repetitive behaviors.
Attention Deficit Disorder
Attention Deficit Disorder is a disorder marked by an ongoing pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development.
Cerebellar Atrophy is caused by degeneration of the cerebellum, the part of the brain that coordinates muscle activity. Cerebellar atrophy can result in impaired muscle coordination, a loss of balance, unsteady gait, slurred speech, difficulty swallowing or chewing, and blindness.
MISDIAGNOSING KAND
Because spasticity, epilepsy and hypotonia are common symptoms, medical professionals often mistake KAND for cerebral palsy or other more common diseases. Additionally, KIF1A mutations have been identified in several other disease studies, highlighting the symptom overlap of KAND with other developmental or degenerative disorders.

If you believe you have an incorrect diagnosis, you must seek genetic testing to receive a correct diagnosis and appropriate care. Because KAND is neurodegenerative, we don’t have time to wait. An incorrect diagnosis could impact the progressive nature of KAND.